Parathyroid adenoma detection in 2016
Hyperparathyroidism is most commonly due to parathyroid adenomas or carcinomas. These can frequently be detected with dual phase Sestamibi scans. The sensitivity for detection is poor with planar and SPECT imaging (60-80%) but with the advent of SPECT-CT much higher sensitivities have been achieved (>85%). Multi-glandular disease is uncommon but paradoxically more difficult to detect with all modalities.
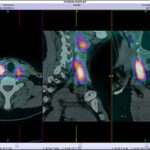
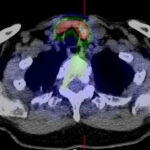
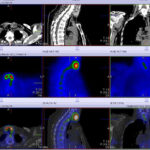
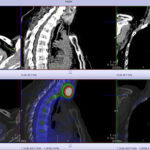
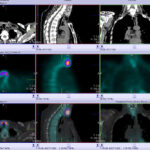
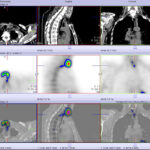
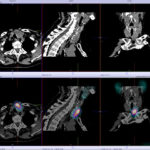
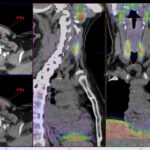
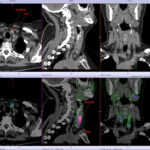
Now with the extra benefit of xSPECT-CT sestamibi scans* small lesions at the lower threshold of resolution for technetium scanning can still be identified when there is a clear corresponding lesion seen on CT.
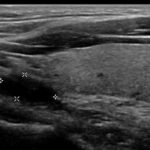
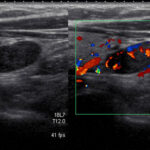
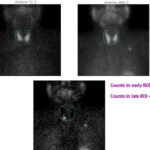
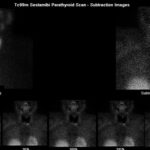
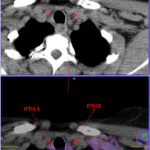
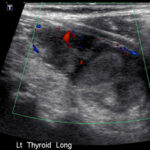
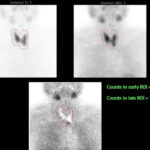
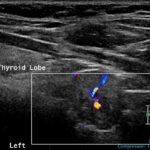
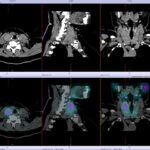
In the author’s experience the best accuracy results from xSPECT-CT using our own specialised uptake threshold mapping and direct quantitative measurement and washout of tracer over 2 sequential scans 2-3hrs apart. We can locate smaller lesions and those lesions with less uptake. This is followed by a targeted ultrasound done so that both modalities can be directly correlated. This allows 3 modality assessment which has reduced the number of negative scans, increased the detections of small lesions, and increased the detection of multiglandular disease. An example of a parathyroid adenoma is seen here. See the parathyroid scan gallery below for more examples.
For those who have negative ultrasounds and SPECT-CT a 4D CT scan of the neck is the next choice (also available at Garran Medical Imaging).
For an overview on hyperparathyroidism and its imaging see an excellent medscape synopsis.
Iain Duncan.
* The xSPECT quantitative sestamibi scans are not widely available and have been developed by Garran Medical Imaging.